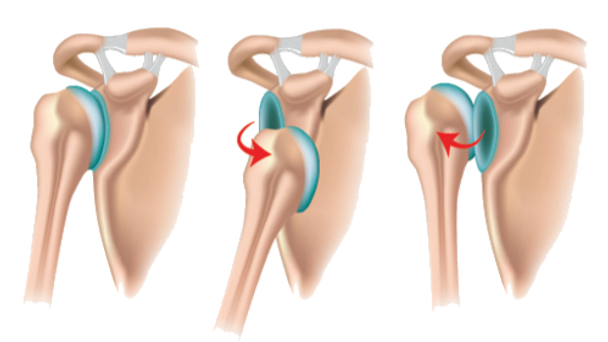
There are three types of dislocation of the shoulder:-
-
Anterior – commonest
-
Posterior
-
Luxatio erecta
1. Anterior Dislocation-
In this dislocation, the head of the humerus comes out of the glenoid cavity and lies anteriorly.
Mode of injury: falling on an outstretched hand with the arm in abduction and external rotation.
It is of three types –
(a). Subcoracoid – The dislocated humoural head comes to lie anteriorly below the coracoid process.
It is the commonest type of dislocation of the shoulder.
(b). Sub glenoid – The humeral head passes through the lower part of the capsule and remains under the glenoid cavity.
(c). Sub clavicular – The head of the humerus occupies a position just below the clavicle.
2. Posterior dislocation –
In this injury, the humeral head comes to lie posteriorly, behind the glenoid.
Mode of injury: caused by a direct fall in front of the shoulder joint with Adam in internal rotation and adduction.
3. Luxatio Erecta –
In rare cases, the arm is strongly abducted, such as when a person is holding a branch of a tree with an arm in a wide abduction while falling from the tree.
As a result, the humeral head is pushed down underneath the glenoid and the arm is held fixed in a wide abduction and also in elevation.
This type of dislocation is termed luxatio erecta.
Clinical features of the shoulder dislocation
Presenting complaints –
-
Pain
-
Inability to move the affected shoulder.
-
Supporting the affected arm by the other hand.
-
History of fall on an outstretched hand.
-
The patient keeps his/her arm abducted.
On examination –
-
The rounded contour of the shoulder is lost.
-
Adduction is severely restricted.
Duga’s Test – Inability to touch the opposite shoulder.
Hamilton Ruler Test – Because of the flattening of the shoulder, a ruler can be placed on the lateral side of the arm. This strikes both the acromion and the lateral condyle of the humerus at the same time.
Call-way Test – When a shoulder dislocates, the vertical circumference of the axilla increases in comparison to the normal side.
Treatment –
Treatment of acute dislocation is reduced by Kocher’s Manoeuver, followed by immobilisation by adduction and internal rotation. The hand of the affected side is close to the opposite shoulder for three weeks.
Occupational therapy management –
OT Aim:-
-
To regain the full active range of movements of the shoulder complex.
Week 1 – 3:- (During immobilisation)
-
Active range of motion exercises of the distal joints such as wrist and fingers.
-
Isometric contraction of the deltoid, biceps and triceps.
After 3 weeks:-
-
The strapping is removed and the limb is supported on a sling.
-
The elbow joint is mobilised to the full extent by removing the sling intermittently.
-
Mobilisation of the shoulder is done in the following ways –
(a). Flexion and extension – with the arm in the sling, a small range of pendulum exercises with the patient in a forward stoop position is begun.
(b). Abduction and external rotation – the initial goal is to achieve related to passive abduction of 45°. It is done with the patient supine and the arm in internal rotation. The therapist passively carries out the abduction at 45°.
Similarly, with the arm in adduction, internal rotation is initiated.
– Self–assisted relaxed movements with a bend in supine lying are also helpful.
– Self-registered isometric and slow isotonic movements should be taught as a home treatment program.
– Heavy resistive exercise, passive stretching and forced external rotation and abduction are safe after 12 weeks.
Activities –
-
Finger ladder
-
Horizontal sanding
-
Bilateral sanding
-
Unilateral sanding
-
Shoulder wheel